
Section outline
-
-
Students mustMark as done
Objectives and outcomes
This topic will help achieve the following
Recognize the value of nutrition assessment in the comprehensive care of ambulatory and hospitalized patients.Demonstrate how to interpret physical findings that reflect nutritional status, including body mass index, waist circumference, growth and development, and signs of nutritional deficiency.Identify the most common physical findings associated with vitamin/mineral deficiencies or excesses.
List the laboratory measurements commonly used to assess the nutritional status of patients. -
Students mustMark as done
Video Tutorial
-
Students mustMark as done
Study Materials
-
-
Students mustMark as done
-
Students mustMark as done
-
Students mustMark as done
-
Students mustMark as done
Pellagra is caused by niacin deficiency and affects primarily the skin, gastrointestinal tract, and nervous system.
-
Students mustMark as done
Malnutrition can affect all areas of the nervous system. Risk factors for malnutrition include alcohol abuse, eating disorders, older age, pregnancy, homelessness, and lower economic status. Any medical condition that affects the GI tract can also impair absorption of essential vitamins. Nutritional deficiencies have been described in patients with inflammatory bowel disease, fat malabsorption, chronic liver disease, pancreatic disease, gastritis, and small bowel resections. Patients receiving total parental nutrition (TPN) are also at risk for vitamin deficiency and TPN formulations should be carefully formulated to include supplemental vitamins and trace minerals. Neurological complications following gastric bypass surgery are increasingly recognized. Nutritional neuropathies manifest either acutely, subacutely, or chronically. They can be either demyelinating or axonal. A unique class of peripheral neuropathy with coexistent myelopathy, also called myeloneuropathy, can also been seen with nutritional neuropathies. Myeloneuropathy has been described with deficiencies of vitamin B12 and copper. Patients with myeloneuropathy will present with both upper motor neuron and lower motor neuron signs. Peripheral neuropathy may mask the symptoms and signs of the myelopathy presenting a diagnostic challenge. Hyper reflexia may be difficult to assess in the presence of severe peripheral neuropathy and ankle jerks may be absent. Muscle weakness may impair the toe extensors, so Babinski sign may not be present. Besides spinal cord/cauda equina arteriovenous malformation, the clinician should suspect myeloneuropathy when the predominant complaint is gait impairment or bowel or bladder dysfunction in the setting of a peripheral neuropathy.
-
Students mustMark as done
Forum

-
-
Students mustMark as done
Case-study Assignment Submission

-
Students mustMark as done
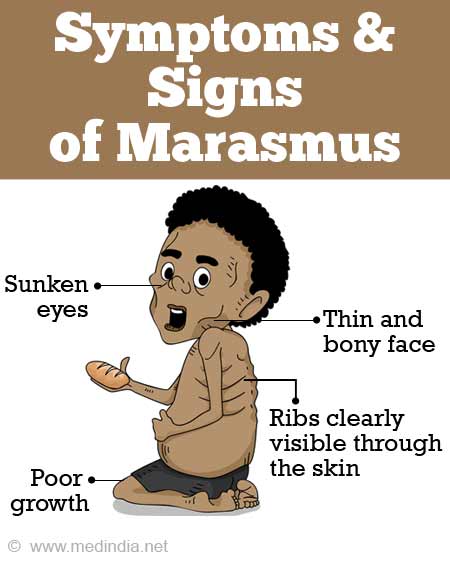
RD is an 8-year-old boy of Liberian descent who lives in the United States with his parents. In October, RD and his family flew to Liberia to spend a few months with their extended family. Several weeks after his arrival, political unrest erupted. RD and his family were forced from their homes at gunpoint, taken to a university, and held against their will in overcrowded, unsanitary conditions. Medical and food supplies were scarce. Food was provided by soldiers outside the camp who lowered buckets of rice and occasionally fish over the barbed-wire fences. Daily tea was also provided. Many of the hostages died from starvation. RD and his family escaped after 3 months of captivity and sought refuge in the American Embassy. From there, they were airlifted to a neigh- boring country. Shortly thereafter, RD returned to the United States.
-

